|
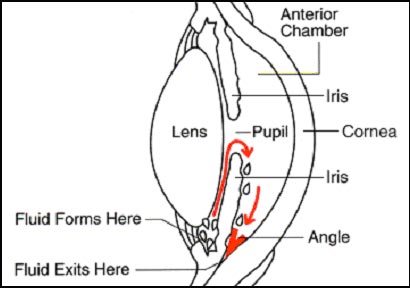
The fluid leaves the
anterior chamber at the angle where the cornea and iris meet (see
diagram). When the fluid reaches the angle, it flows through a spongy
meshwork, like a drain, and leaves the eye.
Open-angle glaucoma gets
its name because the angle that allows fluid to drain out of the anterior
chamber is open. However, for unknown reasons, the fluid passes too
slowly through the meshwork drain. As the fluid builds up, the pressure
inside the eye rises. Unless the pressure at the front of the eye is
controlled, it can damage the optic nerve and cause vision loss.
What are
the symptoms of glaucoma?
At first, open-angle
glaucoma has no symptoms. Vision stays normal, and there is no pain. As
glaucoma remains untreated, people may notice that although they see things
clearly in front of them, they miss objects to the side and out of the
corner of their eye.
Without treatment, people
with glaucoma may find that they suddenly have no side vision. It may seem
as though they are looking through a tunnel. Over time, the remaining
forward vision may decrease until there is no vision left.
How is
glaucoma detected?
Most people think that they
have glaucoma if the pressure in their eye is increased. This is not always
true. High pressure puts you at risk for glaucoma. It may not mean that you
have the disease.
Whether or not you get
glaucoma depends on the level of pressure that your optic nerve can tolerate
without being damaged. This level is different for each person.
Visual acuity:
This eye chart test measures how well you see at various distances.
Visual Field:
This test measures your side (peripheral) vision. It helps your eye care
professional find out if you have lost side vision, a sign of glaucoma.
Pupil dilation:
This examination provides your eye care professional with a better view of
the optic nerve to check for signs of damage. To do this, your eye care
professional places drops into the eye to dilate (widen) the pupil. After
the examination, your close-up vision may remain blurred for several hours.
Tonometry:
This standard test determines the fluid pressure inside the eye. There are
many types of tonometry. One type uses a purple light to measure pressure.
Another type is the "air puff," test, which measures the resistance of the
eye to a puff of air.
Can glaucoma be treated?
Yes. Although you will
never be cured of glaucoma, treatment often can control it. This makes early
diagnosis and treatment important to protect your sight. Most doctors use
medications for newly diagnosed glaucoma; however, new research findings
show that laser surgery is a safe and effective alternative.
Glaucoma
treatments include:
Medicine:
Medicines are the most common early treatment for glaucoma. They come in the
form of eyedrops and pills. Some cause the eye to make less fluid. Others
lower pressure by helping fluid drain from the eye.
Glaucoma drugs may be taken
several times a day. Most people have no problems. However, some medicines
can cause headaches or have side effects which affect other parts of the
body. Drops may cause stinging, burning, and redness in the eye. Ask your
eye care professional to show you how to put the drops into your eye. In
addition, tell your eye care professional about other medications you may be
taking before you begin glaucoma treatment.
Many drugs are available to
treat glaucoma. If you have problems with one medication, tell your eye care
professional. Treatment using a different dosage or a new drug may be
possible.
You will need to use the
drops and/or pills as long as they help to control your eye pressure. This
is very important. Because glaucoma often has no symptoms, people may be
tempted to stop or may forget to take their medicine.
Laser surgery (also
called laser trabeculoplasty):
Laser surgery helps fluid
drain out of the eye. Although your eye care professional may suggest laser
surgery at any time, it is often done after trying treatment with medicines.
In many cases, you will need to keep taking glaucoma drugs even after laser
surgery.
Laser surgery is performed
in an eye care professional's office or eye clinic. Before the surgery, your
eye care professional will apply drops to numb the eye.
As you sit facing the laser
machine, your eye care professional will hold a special lens to your eye. A
high-energy beam of light is aimed at the lens and reflected onto the
meshwork inside your eye. You may see flashes of bright green or red light.
The laser makes 50-100 evenly spaced burns. These burns stretch the drainage
holes in the meshwork. This helps to open the holes and lets fluid drain
better through them.
Your eye care professional
will check your eye pressure shortly afterward. He or she may also give you
some drops to take home for any soreness or swelling inside the eye. You
will need to make several followup visits to have your pressure monitored.
Once you have had laser
surgery over the entire meshwork, further laser treatment may not help.
Studies show that laser surgery is very good at getting the pressure down.
But its effects sometimes wear off over time. Two years after laser surgery,
the pressure increases again in more than half of all patients.
Conventional surgery:
The purpose of surgery is to make a new opening for the fluid to leave the
eye. Although your eye care professional may suggest it at any time, this
surgery is often done after medicine and laser surgery have failed to
control your pressure.
Surgery is performed in a
clinic or hospital. Before the surgery, your eye care professional gives you
medicine to help you relax and then small injections around the eye to make
it numb.
The eye care professional
removes a small piece of tissue from the white (sclera) of the eye. This
creates a new channel for fluid to drain from the eye. But surgery does not
leave an open hole in the eye. The white of the eye is covered by a thin,
clear tissue called the conjunctiva. The fluid flows through the new
opening, under the conjunctiva, and drains from the eye.
You must put drops in the
eye for several weeks after the operation to fight infection and swelling.
(The drops will be different than the eyedrops you were using before
surgery.) You will also need to make frequent visits to your eye care
professional. This is very important, especially in the first few weeks
after surgery.
In some patients, surgery
is about 80 to 90 percent effective at lowering pressure. However, if the
new drainage opening closes, a second operation may be needed. Conventional
surgery works best if you have not had previous eye surgery, such as a
cataract operation.
Keep in mind that while
glaucoma surgery may save remaining vision, it does not improve sight. In
fact, your vision may not be as good as it was before surgery.
Like any operation,
glaucoma surgery can cause side effects. These include cataract, problems
with the cornea, inflammation or infection inside the eye, and swelling of
blood vessels behind the eye. However, if you do have any of these problems,
effective treatments are available.
What are
some other forms of glaucoma?
Although open-angle
glaucoma is the most common form, some people have other forms of the
disease.
In low-tension or
normal-tension glaucoma, optic nerve damage and narrowed side vision occur
unexpectedly in people with normal eye pressure. People with this form of
the disease have the same types of treatment as open-angle glaucoma.
In closed-angle glaucoma,
the fluid at the front of the eye cannot reach the angle and leave the eye
because the angle gets blocked by part of the iris. People with this type of
glaucoma have a sudden increase in pressure. Symptoms include severe pain
and nausea as well as redness of the eye and blurred vision. This is a
medical emergency. The patient needs immediate treatment to improve the
flow of fluid. Without treatment, the eye can become blind in as little as
one or two days. Usually, prompt laser surgery can clear the blockage and
protect sight.
In congenital glaucoma,
children are born with defects in the angle of the eye that slow the normal
drainage of fluid. Children with this problem usually have obvious symptoms
such as cloudy eyes, sensitivity to light, and excessive tearing. Surgery is
usually the suggested treatment, because medicines may have unknown effects
in infants and be difficult to give to them. The surgery is safe and
effective. If surgery is done promptly, these children usually have an
excellent chance of having good vision.
Secondary glaucomas can
develop as a complication of other medical conditions. They are sometimes
associated with eye surgery or advanced cataracts, eye injuries, certain eye
tumors, or uveitis (eye inflammation). One type, known as pigmentary
glaucoma, occurs when pigment from the iris flakes off and blocks the
meshwork, slowing fluid drainage. A severe form, called neovascular
glaucoma, is linked to diabetes. Also, corticosteroid drugs—used to treat
eye inflammations and other diseases--can trigger glaucoma in a few people.
Treatment is with medicines, laser surgery, or conventional surgery. |